If you know me, then you know that I my goal is to get bananas off the potassium handout. And by that I mean, I want to shift the focus of low potassium diets away from fruits and vegetables.
I think the first step for low potassium diet teaching should focus on other high potassium food sources. There is a list of these high potassium food sources in my hyperkalemia assessment checklist. Check it out if you haven’t already.
But does that mean that I think there is no link between fruit and vegetable intake and hyperkalemia?
What do we know about potassium in fruits and vegetables?
My first scientific paper was: Potassium additives and bioavailability: are we missing something in hyperkalemia management?

In this paper I discuss the results of this study, which investigate the bio-accessibility of potassium in fruits and vegetables. This paper blew my mind!
The easy take away is the potassium from whole plant foods is less bioavailable than animal foods. Specifically, the potassium bio-accessibility in the diet made up mostly of whole, unprocessed plant foods was 76.8%. Compared to 96.3% for a diet made up of processed fruits and vegetables and animal products.
So does that mean that we don’t need to worry about whole, minimally processed plant foods at all? That they never cause hyperkalemia?
No, not exactly. Consider that lower bioavailability doesn’t mean zero bioavailability.
In Stage 3 CKD high potassium DASH-style diets are associated with hyperkalemia
In this study adults living with Stage 3 CKD were fed both a high potassium (4000mg) and a low potassium (1600mg ) diet over a 4 week period. And while the authors don’t provide the exact menus, they describe the higher potassium diet as a DASH style diet. Specifically emphasizing fruits and vegetables, low fat dairy, whole grains, nuts and seeds.
Based on the work, of this paper, we anticipate that the potassium bio-accessibility in DASH-style diets is about 62%. So this would mean that actual amount of available potassium in the high potassium arm is (4000 * 0.62 =) 2480mg.
On average, the serum potassium levels were 0.2mmol/L higher during the high potassium diet compared to the low potassium diet. Additionally, when people were eating the high potassium diet, there was 2.5 times greater chance of having hyperkalemia. Two participants had a K above 5.5mmol/L and had to be withdrawn from the high potassium feeding arm.
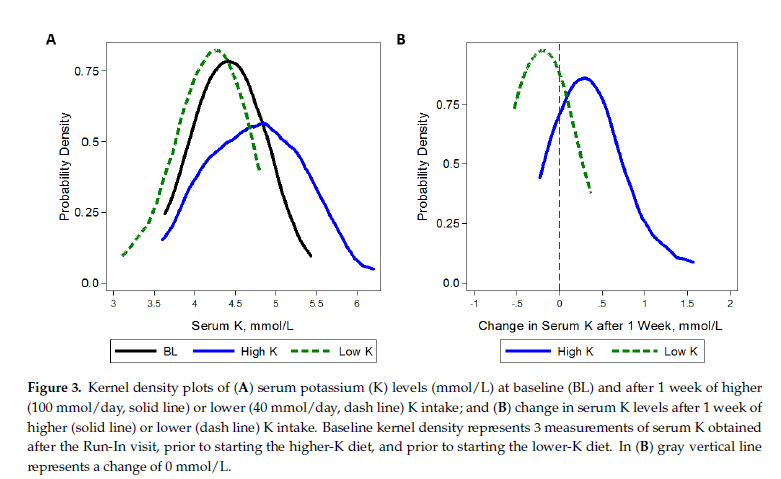
So this paper suggests that despite the lower bioavailability of the high potassium diet – that the increase in potassium intake was enough to increase serum potassium levels and increase the risk of hyperkalemia.
Take Aways
For me, my take aways are:
- Not all potassium sources are equal – some are more likely to increase serum potassium than others
- Even low bioavailable potassium foods can increase potassium levels because low is not the same as none
- For my patients with hyperkalemia, I start by restricting the high bioavailable potassium foods. But, if my patients aren’t consuming any of these foods, then I start searching for high intakes of low bioavailable potassium sources.
Though, I say all of this on caveat that I have completed a thorough hyperkalemia assessment and have decided that diet teaching for potassium is the most appropriate intervention.