Recently I received an email asking about how to interpret a low eGFR in athletes. This is an excellent question because interpreting eGFR results can be incredibly difficult in athletes if they have high muscle mass. Let’s look at why.
How do we calculate eGFR?
eGFR stands for estimated glomerular filtration rate, emphasis on the e. We don’t actually MEASURE kidney function, we estimate it using a marker of kidney function. The marker we use is creatinine. I describe this to my patients as the “waste product that a working kidney would normally get rid of”.
Labs use a formula to calculate eGFR. When I want to calculate eGFR on my own, instead of relying on the labs calculation, I head to the National Kidney Foundation’s website here.
What variables do labs use use to calculate eGFR?
The variables used to calculate eGFR are:
- Serum creatinine (measured as a concentration)
- Age
- Sex
- Body surface area
While age and sex are fairly black and white, both serum creatinine and body surface area can be specific to your patient.
What impacts creatinine values?
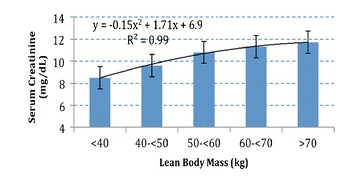
The 2024 KDIGO CKD Guidelines note that creatinine directly correlates with muscle mass in a positive linear relationship. This means that as muscle mass goes up so does the creatinine.
Check out the graph below from a paper published in the Journal of Cachexia, Sarcopenia and Muscle. This graph shows that in people receiving hemodialysis, as the muscle mass goes up, so too does the creatinine.
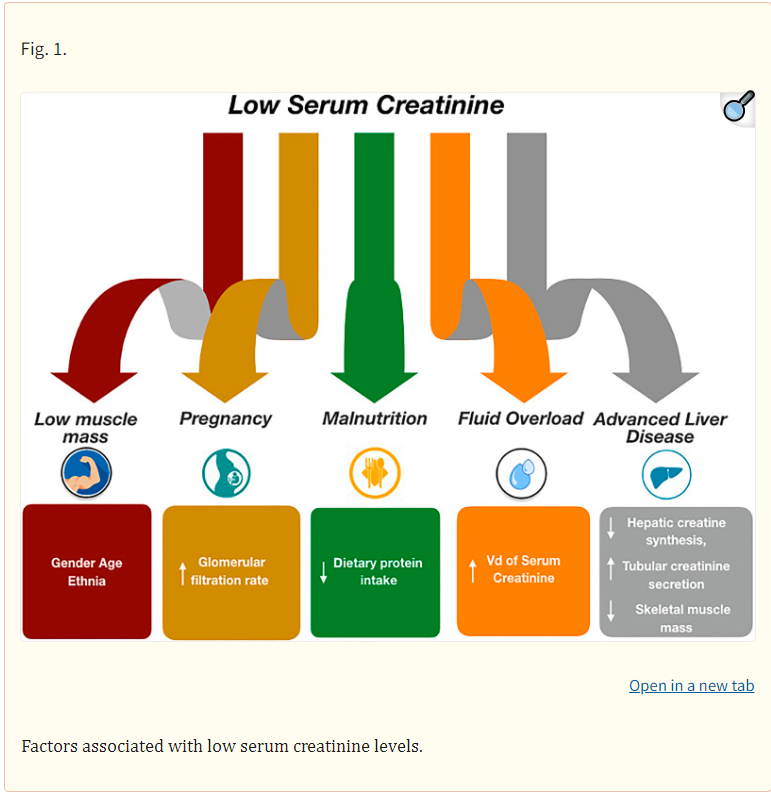
On the flip side, several factors can make creatinine go down. I really liked this figure, which I found in a 2023 paper published in Blood Purification. While this paper discussed factors that can explain low serum creatinine, consider that both muscle mass and volume status can be a 2-way relationship. Both high muscle mass and dehydration can be causes for high serum creatinine too.
What impacts body surface area?
Labs report body surface area using a standard body surface area of 1.73 m². However if your patient’s body size is much larger or smaller than an average person using standard body surface may lead to an incorrect eGFR result.
In these cases, I typically adjust the calculation based on my patients body surface area by using an eGFR calculator.
How should eGFR be calculated for athletes?
In athletes with high muscle mass, adjusting for their body specific surface area may improve the estimation of eGFR, but may still be inaccurate. I think of this as akin to BMI. For those with high muscle mass, who have a high BMI as a result, it is likely that creatinine and standard eGFR calculations will fail to be good indicators of kidney function.
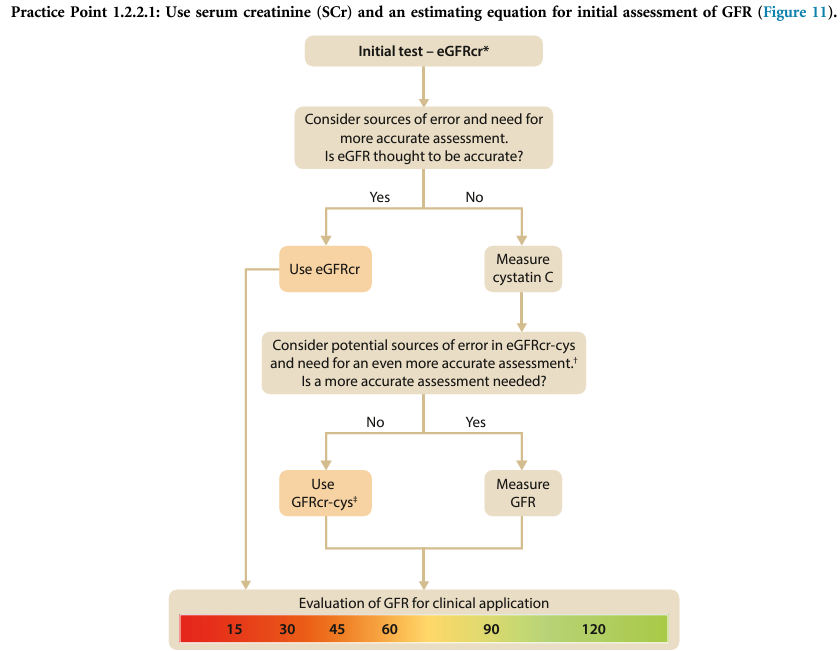
The 2024 KDIGO guidelines note that eGFR calculated using both creatinine and cystatin C can be considered more accurate for evaluating the risk of negative health outcomes related to eGFR when compared to using eGFR calculated with creatinine alone.
So if cystatin C is available, it may be worthwhile to use both Creatinine and Cystatin C to estimate eGFR as per this flow diagram from the 2024 KDIGO guidelines.
Take Aways
- Because high muscle mass increases serum creatinine levels, eGFR may be underestimated in athletes with high muscle mass
- To get a better estimate of eGFR, I would recommend adjusting eGFR calculations based on patient’s body surface area using an eGFR calculator, such as the one available on the National Kidney Foundation Website.
- If a more accurate assessment is needed, and cystatin C is available, using both creatinine and cystatin C to estimate GFR may improve accuracy.
If you are keen to know more, check out my previous post here. More on this topic, including discussions of Cystatin C and protein recommendations for athletes to come.
6 thoughts on “Low eGFR in Athletes”