Johnson RK. Dietary intake–how do we measure what people are really eating?. Obesity. 2002 Nov 1;10(s11):63S.
Taking a diet history is what makes dietitians unique from other healthcare providers. I often tell my students that you will most likely hear all members of the healthcare team give out nutrition advice. But, as dietitians, we are (usually) the only ones that give personalized nutrition advice. Because we take the time to assessment our patients dietary intake.
But – its not as simple as a it seems
That being said, taking a diet history takes skill and can be challenging. It also takes time. And time is precious, as we scramble with higher patient loads and more complex patients.
I am a renal dietitian. So often I am doing a diet history to figure out if someone is eating excess potassium or phosphorus. And it wouldn’t be uncommon for me to find a stack of 7 hyperkalemia referrals in my mailbox each day.
But sometimes, I do my diet history and I am still stumped. Nothing that my patients are eating appears to be too high. Or I am left with the impression that my patients eat healthier than I do.
So, what am I missing? (And – disclaimer alert – sometimes hyperkalemia isn’t related to diet – but more on that in another post).
Bring in the continuing competency
A few years ago, as part of my continuing competencies for my college registration I reviewed dietary assessment techniques. I discovered that my normal ways of going about my diet history were, quite honestly, not that great.
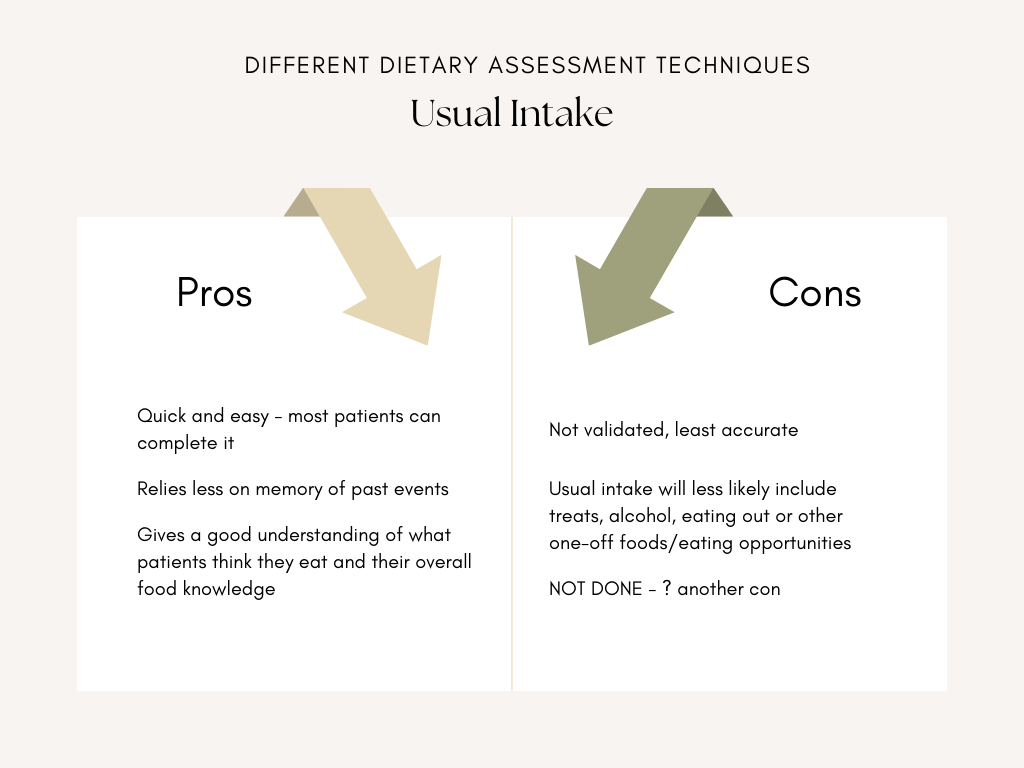
I often asked my patients about what they usually ate? What do you usually have for breakfast? What do you usually have for lunch? You get the idea…
But here’s the thing – when patient’s describe their usual intake, they give us their ideal day. And I hope I am not alone here (eating cookies as I type this – an unexpected gift from my neighbour) that despite all of our best efforts, sometimes extra foods slip in and we deviate from our “usual” or “ideal” diets. I think that is what makes us human, and my patients are humans too… not robots. Robots are much better at sticking to ideal than humans.
The Article
So I came across this article “Dietary intake-how do we measure what people are really eating?” published in the Journal of Obesity in 2002. I know its an old one – but honestly, there aren’t many articles in the literature that are aimed at dietary intake assessments in clinical practice.
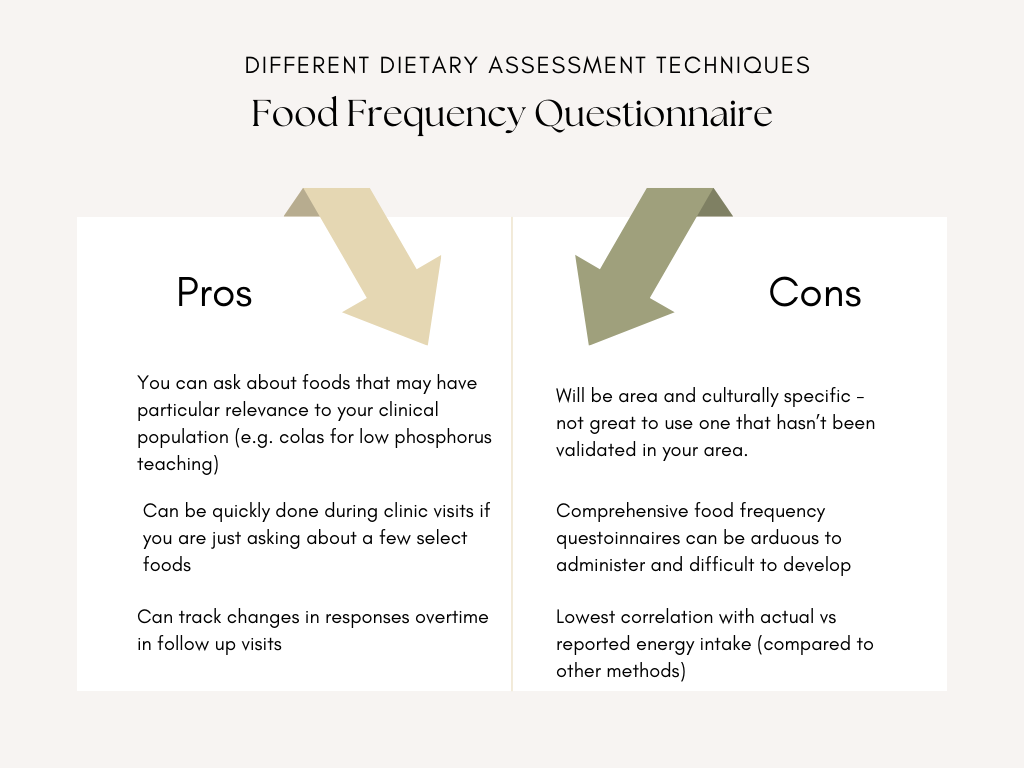
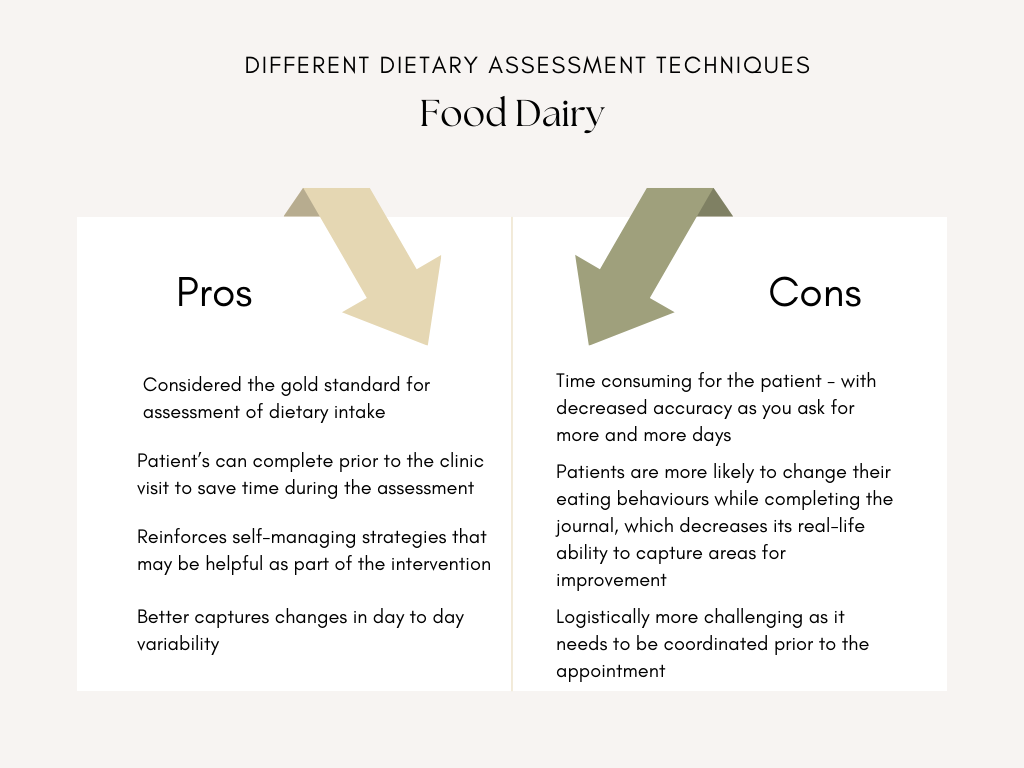
The article outlines a few of the pros and cons of the different assessment methods and I added a few of my own two cents too.
My Own personal take aways
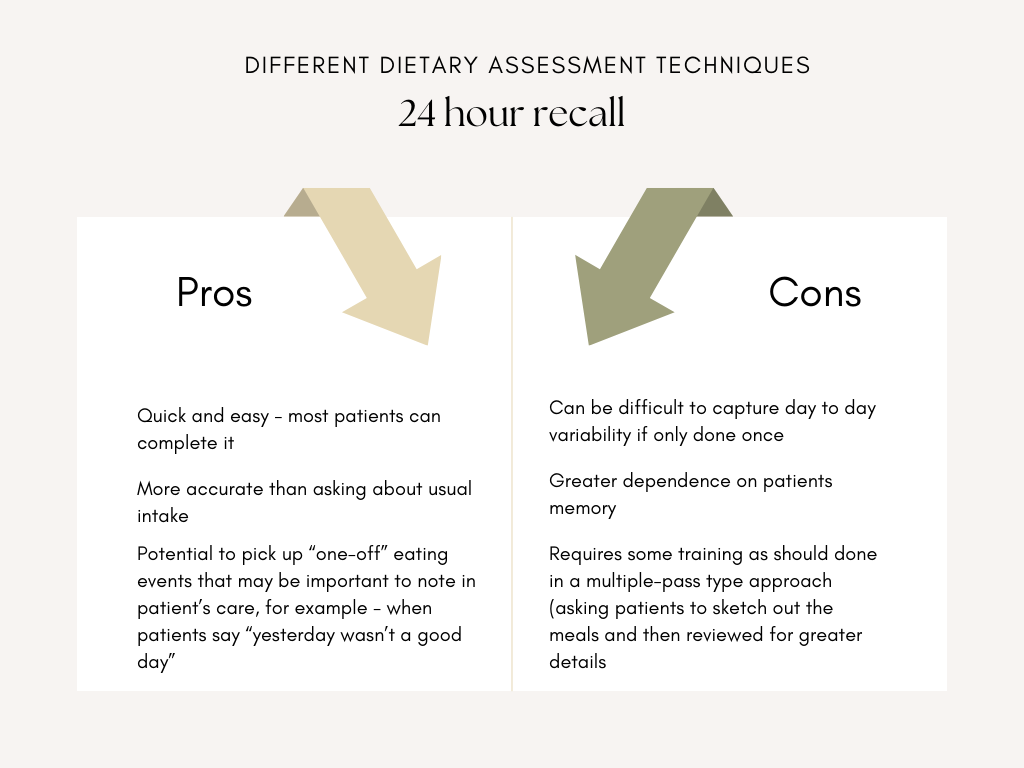
- My preferred dietary assessment technique is a multiple pass 24 hour recall
- I often ask about usual intake too. I do this to see how usual intake differs from the 24 hour recall. But usual intake only replaces a 24 hour recall if my patient has memory problems
- As I get to see my patients more than once, I also keep track of how often they tell me “Yesterday wasn’t a good day”. Because I think this can give me a clue as to how often they might be deviating from their usual/ideal state


One thought on “Dietary intake-how do we measure what people are really eating?”