
I want to develop a metabolic acidosis nutrition assessment cheat sheet, similar to my one for hyperkalemia, so I am digging down the rabbit hole of acid/base balance in CKD. Adults living with CKD are at increased risk of accumulating excess acid and developing a condition known as metabolic acidosis.
Metabolic acidosis in CKD is important because, there is growing interest and recognition that:
- Correcting metabolic acidosis helps preserve kidney function
- That what adults living with kidney disease eats impacts metabolic acidosis
So in today’s post I am going through a 2021 review about metabolic acidosis in CKD.
What is metabolic acidosis and why do adults with CKD get it?
Metabolic acidosis is common in kidney disease. Kidney’s are responsible for helping to maintain pH balance but eliminating ammonia in the urine. The process of eliminating hydrogen ions through ammonia, helps the body preserve it’s supply of bicarbonate ions. Bicarbonate ions are then used to neutralize acids produced by the body through normal metabolic processes.
Phew, that’s complicated. Let’s break that down:
- Step 1: Pee out ammonia
- Step 2: This allows for bicarbonate recycling
- Step 3: Bicarbonate is then available to pick up other acids produced in the body
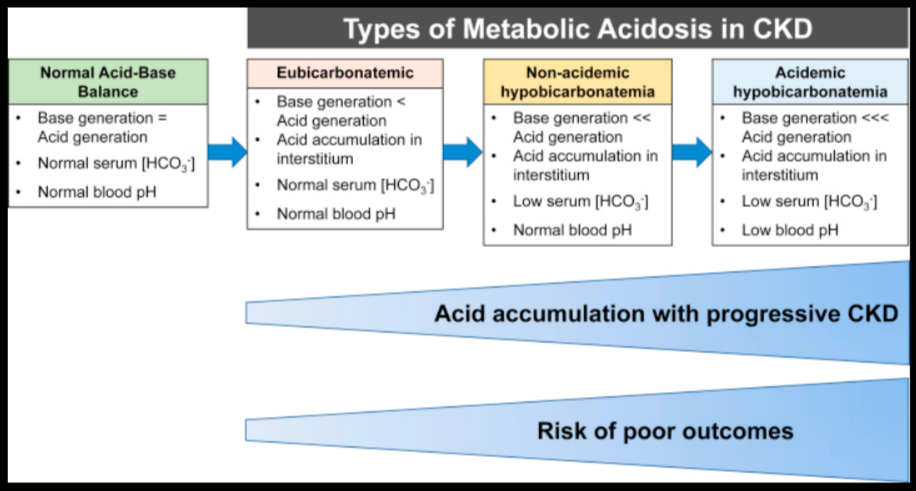
The authors of the article describe metabolic acidosis in CKD as a spectrum, ranging from undetectable changes in ammonia secretion but otherwise normal lab values, all the way to low serum bicarbonate coupled with low blood pH.
Why do we care about metabolic acidosis?
The concerns with metabolic acidosis include:
- Decreased bone health
- Reduced muscle health
- Accelerated eGFR decline
- Increased risk of death
Does correcting metabolic acidosis stop these bad things from happening?
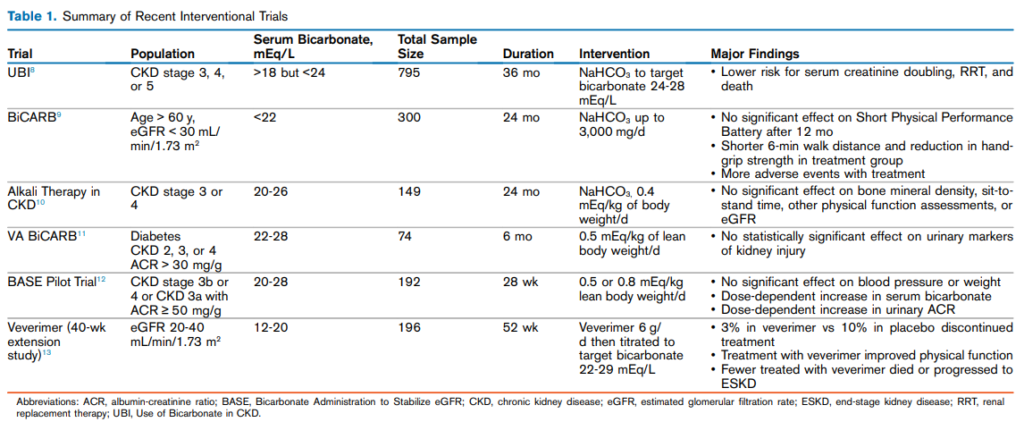
While some trials investigating sodium bicarbonate tablets to correct metabolic acidosis have reported improvements in metabolic outcomes, such as a lower risk for increasing creatinine, other studies investigating sodium bicarbonate on bone and muscle parameters have failed to demonstrate clear benefit.
The authors propose that one reason is that trials to date may not be correcting acidosis sufficiently to achieve benefit. In fact, doses up to 4.1g per day have been studies and in these higher dose studies, the effects appear to be better.
When should acidosis be treated?
It is recommended to target a serum bicarbonate level of 22mEq/L or higher. Though newer studies are starting treatment at 24mEq/L. It is suggested to have a repeat value before starting treatment.
Take Aways
This article provided some nice background on metabolic acidosis, though didn’t cover anything to do with diet.
So while I am convinced that we should treat metabolic acidosis, I am still wondering what role diet has in correcting acidosis? Clearly – more to come!
One thought on “Backgrounder on Metabolic Acidosis in CKD”