I received this question from a colleague of mine who was wondering if we should start including potassium:fibre ratios.
There have been a few studies published that have started to discuss this topic, including this one and this one.

Why is fibre recommended?
Fibre may have particular benefit for adults living with kidney disease. According this review article, fibre can help:
- Increase Stool Output
- Improve gut microbioata
- Improve the gut barrier
- Decrease Inflammation
- Decrease uremic toxin production
All of these seem like good reasons to encourage adults living with CKD to consume more fibre. However, as the authors point out, traditional dietary potassium restrictions, which tend to restrict fruit and vegetables, whole grains and plant proteins likely make it challenging for this population to consume adequate fibre.
Is higher fibre intake associated with improvements in serum potassium levels?
Given the potential for fibre to increase stool volume and (as I highlight in my hyperkalemia assessments) we poop out a lot of potassium, there is a theoretical link that consuming more fibre result in lower serum potassium levels.
However, according to this 2-year prospective study done in children living with CKD, those who consumed more fibre didn’t have lower serum potassium levels.

Strengths of the Study: The researchers used validated diet tools. 24 hour recalls and 3 day food records were used to estimate dietary fibre and potassium intake. Serum potassium values were also measured at these visits. 52 children completed the study. There was a clear link between potassium intake and fibre. As potassium increased, so did the fibre. There was no association between potassium intake or fibre intake and serum potassium levels.
Limitations of the Study: Here is where it is good to check the methods sections of the paper. The children had eGFRs between 25-68, with a mean eGFR of 49. Consider that urinary potassium excretion tends to be preserved until after Stage 3B. Therefore, it is possible that the reason this study failed to see a relationship was that the participants had normal renal potassium handling.
Future Studies: Investigating the relationship between potassium and fibre intake and circulating potassium levels are recommended in later stage CKD to better assess the relationship.
And here’s good news – it looks like there is currently a study underway at the University of Nevada. I will be watching for that publication to come out!
Do foods with higher K:Fibre ratios have lower potassium bioavailability?
We don’t really know. Unfortunately, there isn’t much evidence one way or another. This article investigated the bioavailability of potassium from different plant foods. They used a “test tube digestion” method. The authors reported there were significant differences in bioavailability of potassium from plants. Unfortunately, they didn’t comment on the fibre content.
But fear not, I like math. I looked up the fibre content of each of these food items in the Canadian Nutrient File. Then calculated a potassium to fibre ratio. One interesting thing I came across, was that the Canadian Nutrient File reported significant differences in potassium content than the article (see graph below). For all numbers this is the potassium and fibre content per 100g of raw material.
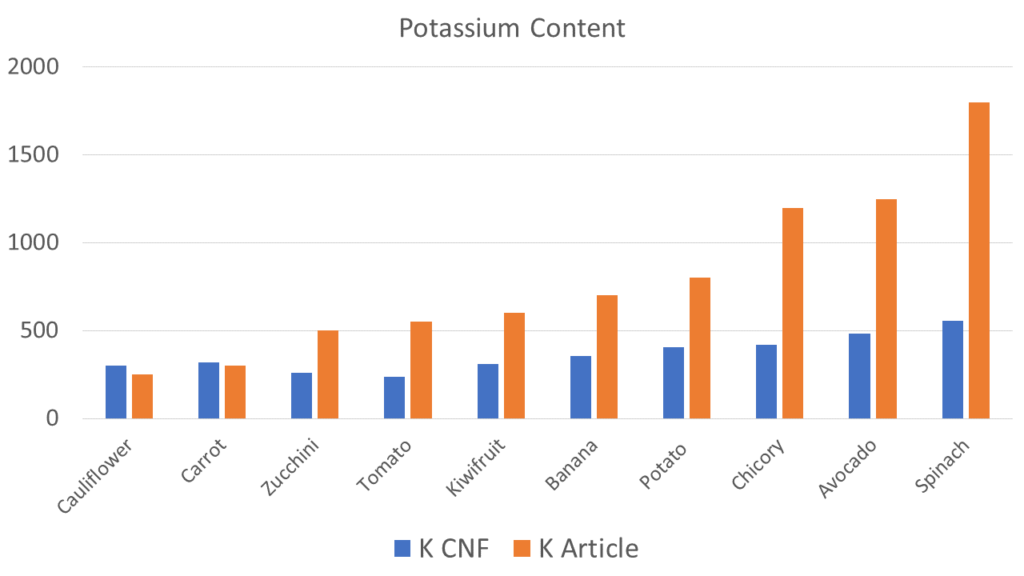
Why there are such differences I don’t know. I could hypothesize that it has to do with the growing locations of some of the foods, the ripeness of some of the foods or the methods used to determine the potassium content. Either way – the point is that potassium content isn’t static and even with great resources like the Canadian Nutrient File, it’s possible there is some misreporting.
Potassium:Fibre Ratio Calculations
Because of the difference in reported potassium content, I calculated two potassium:fibre ratios. One using the numbers from the Canadian Nutrient File. And one with the potassium numbers from the article. Fibre wasn’t reported, so for both I used the fibre numbers from the Canadian Nutrient File. I could not see that there was association between the reported bioavailablity and the K:Fibre ratio regardless of which ratio was used..
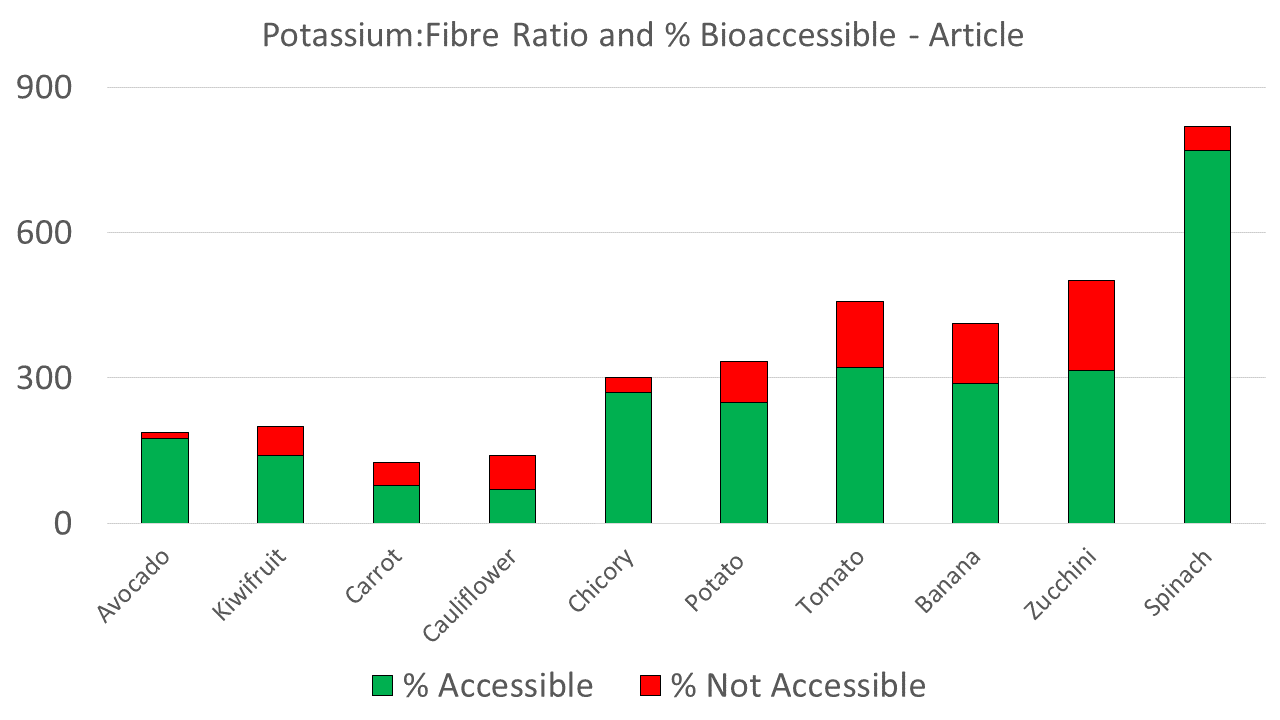
There are the numbers for the articles reported potassium content and the fibre ratio calculated from this number. What this graph shows is that despite increasing K:Fibre ratios, the % accessible/not accessible isn’t moving in a predictable way. For example avocado has a great K:Fibre ratio but had really high bioaccessibility. Zucchini had a “bad” K:Fibre ratio but actually had relatively low bioaccessibility at only 63%.
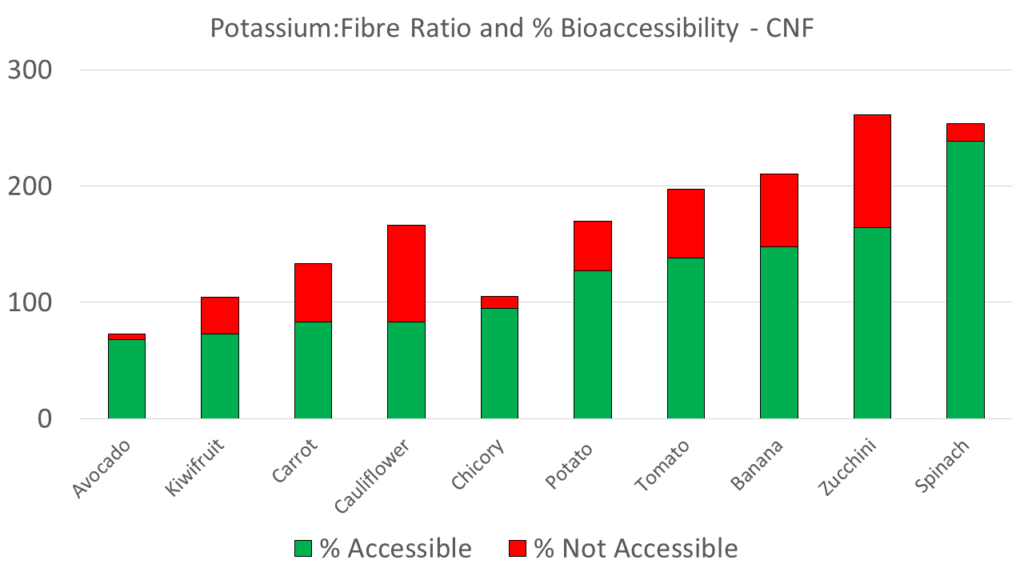
While the ratio is difference using the data from the CNF, again the pattern isn’t predictable and the final ordering of bioaccessibility didn’t change. This leads me to believe that the failure to see a relationship is unlikely related to misreporting of potassium content.
Of course – this is only one study and a limitation is test-tube digestion vs real digestion. Not to mention that humans might eat these foods in mixed meals which will likely impact bioavailability too.
Take Aways
While I completely agree that fibre is an important nutrient, I am not sure how talking to patients about a potassium:fibre ratio adds benefit.
At the end of the day, really I just want my patients to eat more plants. So with the exception of my keenest patients, I can’t see me teaching this concept very often. And if I want to talk about fibre with my patients, I wonder if a simple fibre handout would work just as well.