
My favourite topic – Hyperkalemia! There are some excellent points in this section.
For repeat visitors to my blog, you will know that:
- Kidneys are important for maintaining normal serum potassium values
- Lots of different things can impact potassium levels
So let’s dive into the KDIGO recommendations!
What are the recommendations?

Practice Point 3.11.5.1: Implement an individualized approach in people with CKD G3–G5 and emergent hyperkalemia that includes dietary and pharmacologic interventions and takes into consideration associated comorbidities and quality of life (QoL). Assessment and education through a renal dietitian or an accredited nutrition provider are advised.
Practice Point 3.11.5.2: Provide advice to limit the intake of foods rich in bioavailable potassium (e.g., processed foods) for people with CKD G3–G5 who have a history of hyperkalemia or as a prevention strategy during disease periods in which hyperkalemia risk may be a concern.
What are the risk factors for hyperkalemia?
The risk factors for hyperkalemia outlined in this guideline include:
- Elevated ACR
- Diabetes and hyperglycemia
- Constipation
- Medications
- Acidosis
- Dehydration (hypernatremia)
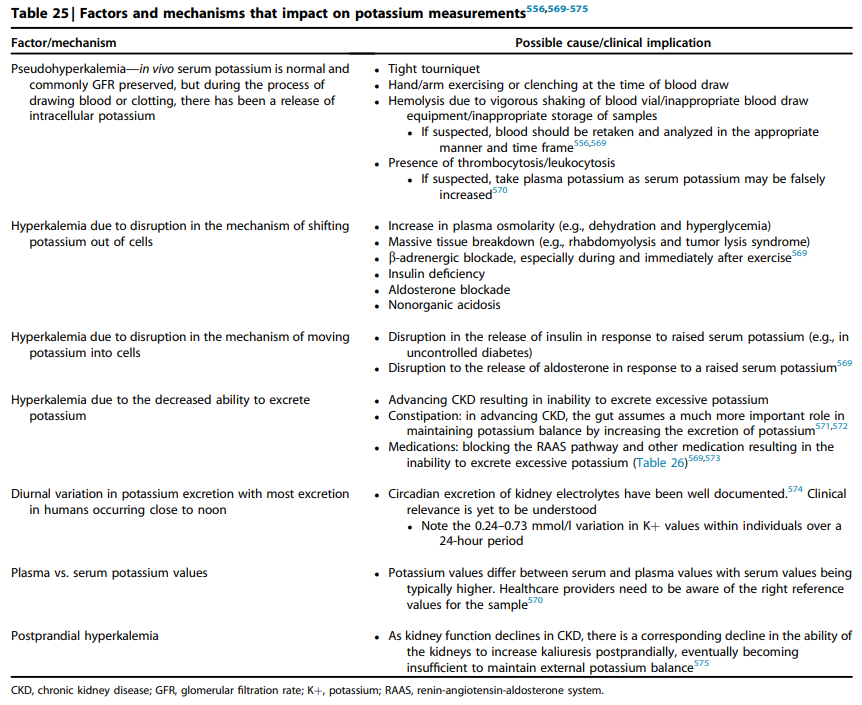
I loved Table 25 in these guidelines and have included a screen shot for you. A great summary of factors impacting potassium balance.
What medications are associated with hyperkalemia?
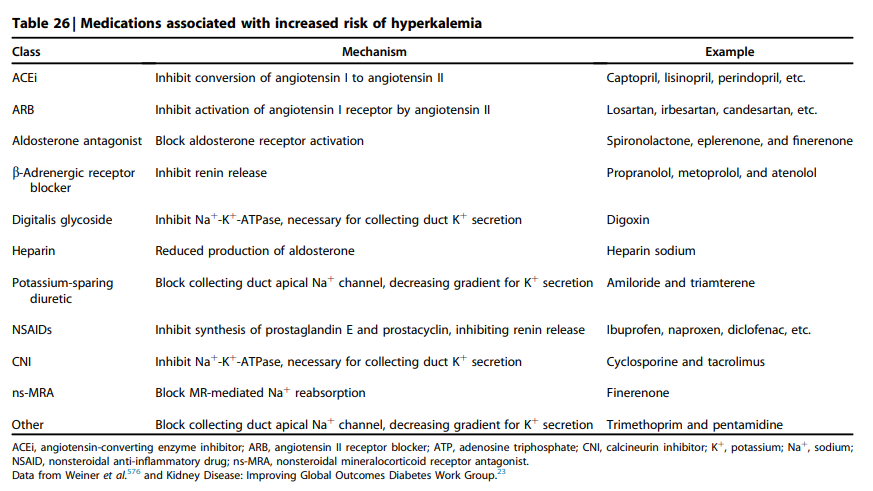
You may want to print table 26 for your resource binders/white boards in your office, as it gives a comprehensive summary of medications associated with hyperkalemia.
When should we treat hyperkalemia?
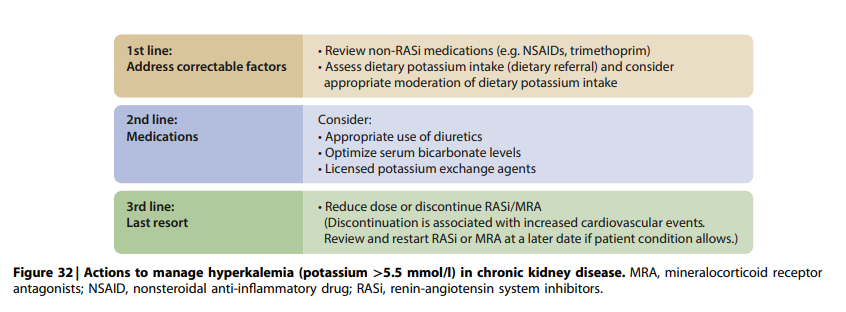
Based on Figure 32, KDIGO doesn’t recommend initiating management strategies for hyperkalemia until potassium is over 5.5mmol/L. There are no other recommendations in the text about when to treat.
They also highlight that there appears to be hyperkalemia-tolerance as CKD advances, as the risk of death related to hyperkalemia decreases in more advanced CKD.
Should people without a history of hyperkalemia or risk factors for hyperkalemia restrict their potassium intake?
Definitely not. The KDIGO group cites one of my systemic reviews (which is super exciting for me!). In this review, we found that in early stages of CKD high potassium intake appears to be protective against disease progression.
So, in early stages of CKD coupled with a low risk of hyperkalemia do not restrict potassium.
What foods should be restricted on a low potassium diet?
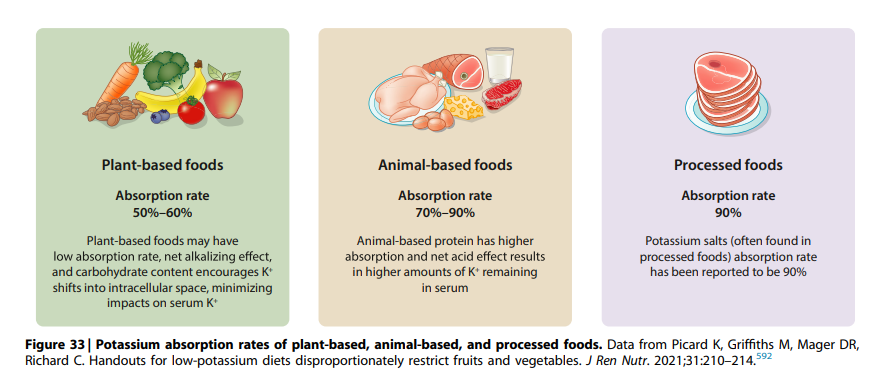
They suggest that restrictions of highly bioavailable potassium may be a supportive prevention strategy for hyperkalemia. The KDIGO guidelines emphasize restriction of highly processed foods, meats, dairy products, and juices as opposed to whole, unprocessed plant foods.
Shout out to my co-authors on this paper, as this a direct citation of our efforts! If you want to know more about this paper, on my blog you can find a video and write up here.
They also highlight the BC Renal Resource for teaching patients about potassium: http://www.bcrenal.ca/resourcegallery/Documents/Potassium_Management_in_Kidney_Disease.pdf
Way to go to the BC Renal Dietitians who worked on this handout! Your amazing work has been praised in these international guidelines!
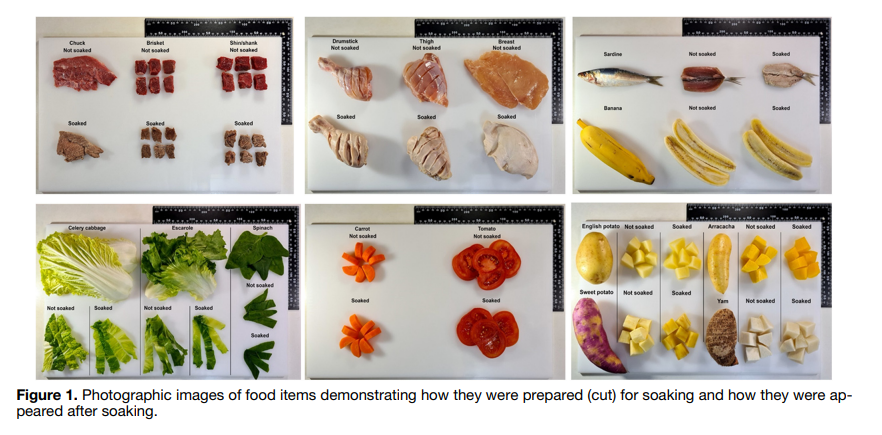
They also discuss soaking foods for 5-10 minutes to help reduce potassium. Ever since I worked on this paper, I often recommend this technique. I have actually printed off the picture from our paper to give to patients so that they understand how to cut the pieces of food for soaking.
Take Aways
I felt very honored to be cited a number of times in this section. Potassium and renal nutrition are deep passions of mine. It is so exciting to see my work being used to make practice recommendations. Thank you KDIGO working group!
If you need help implementing these recommendations, check out my hyperkalemia assessment resource!
A colleague reached out to ask why elevated ACR is considered a risk factor for hyperkalemia. While this isn’t explicitly reviewed in the KDIGO guidelines, my guess would be that elevated ACR is indicating advancing disease progression and this is and of itself would increase the risk of hyperkalemia.